Imagine a healthcare system where the most vulnerable individuals – those struggling with complex medical conditions, behavioral health issues, and inadequate social support – receive the holistic care they deserve. A system that moves beyond treating symptoms and prioritizes long-term well-being, recognizing the impact of housing, employment, and social determinants on health outcomes. This drives Marin County's Whole Person Care program.
Marin County's Whole Person Care program is not just a vision but a tangible effort to build a sustainable, evidence-based, outcomes-focused, coordinated care system across health and social sectors. This program is a testament to the County’s commitment to better serve the most vulnerable Medicaid (Medi-Cal) beneficiaries. It's a beacon of hope for those struggling with complex medical conditions, behavioral health issues, and inadequate social support.
The program’s implementation, funded by federal Medicaid funds matched by local funding, has already made a significant impact in ending chronic and veteran homelessness. The pilot has since become a permanent program within HHS, building upon existing programs and services.
Marin's intervention model focuses on individuals who experience complex medical conditions, behavioral health issues, or lack adequate social support. These factors can interfere with standards of care and result in high utilization and costs.
Marin's care ecosystem has a particular focus on individuals who experience homelessness or who are precariously housed. Their model of care incorporates the following:
- Housing First: A housing-first policy intentionally seeks out chronically homeless individuals with complex health and social issues and first serves those with the highest need.
- Person-Centered Care: Person-centered care is a way of thinking and doing things that sees the people using health and social services as equal partners.
- Trauma-Informed Approach: Trauma-informed care is grounded in and directed by a thorough understanding of the effects of trauma on a person's life and considers its impact on their path to wellness and recovery.
- Social Determinants of Health: This approach focuses on improving an individual's overall wellness rather than simply treating symptoms of illness.
A significant milestone in the Whole Person Care program was the integration of Activate Care’s CareHub platform. This platform facilitates bi-directional information sharing and secure communication among providers. Such information sharing enables systems-level change in new, coordinated, and sustainable ways, proven to meet the needs of high-risk, high-cost Medi-Cal beneficiaries. CareHub’s role in this process is instrumental, providing a robust and secure platform for data sharing and care coordination.
Depending on their needs, clients may enroll in one of three case management programs - housing, medical, or mild-to-moderate mental illness case management. Case managers build a client-centered care plan that includes social determinants of health such as housing, employment, transportation, and education.
Activate Care helps Marin County's care teams share data, collaborate client by client, and expand cross-sector partnerships through the CareHub platform. Through data sharing and the CareHub care coordination platform, 30 partner agencies can access nearly 1,900 client profiles for vulnerable county residents.
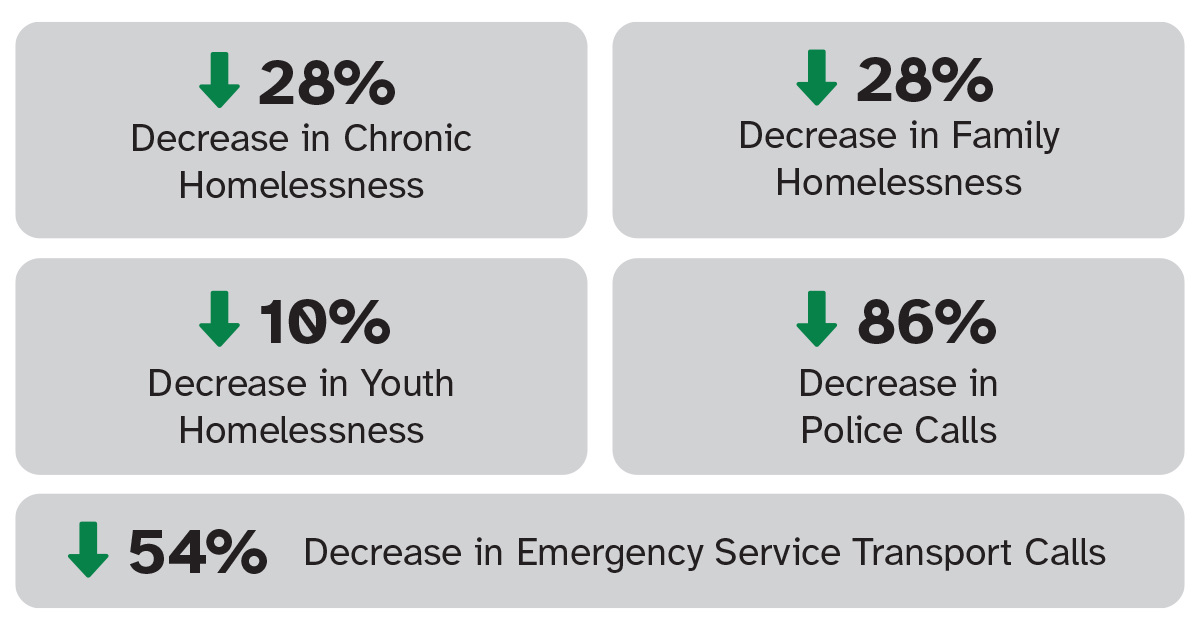
Through their care coordination processes and community engagement strategies, Marin HHS and their partners have achieved the following:
The CareHub all-in-one Platform for SDOH Care is more than just a platform; it's a comprehensive solution for seamless, effective community care management. With a centralized hub, CareHub transcends data management to efficiently streamline client care. It provides a single view into services, programs, and referrals, enhancing the efficiency of care provision. Each client has an individual community care record to track, monitor, report, and, with client permission, share outcomes, thereby enhancing transparency and accountability in care delivery.
Our closed-loop referral system enables seamless coordination and tracking of bi-directional referrals across the community, enhancing communication and shared decision-making and fostering mutual trust in community health programs.
Through workflow automation, team-based tasks and goals, non-medical billing, and integrations, CareHub makes facilitating care easy so you can focus on what matters — improving care for our most vulnerable community members.
Interested in how CareHub can help you better serve your members? Learn more here.